AN EFFECTIVE WAY TO REDUCE CHILDHOOD CARIES: A COMPARISON OF CHILD ORAL HEALTH PROGRAMS IN NEW ZEALAND AND SCOTLAND Download PDF Version
COMPARISON OF IMPROVED CARIES FREE STATUS IN CHILDREN IN NEW ZEALAND AND SCOTLAND
Examination of published data on the Caries Free (CF) status of children in New Zealand and Scotland between 2000 and 2015 shows that Scotland’s children are faring better than those in New Zealand, even though Scotland doesn’t fluoridate its water. Both countries provide free oral health services for children from birth until age 18.
The following charts, based on 2000-2015 published data, compare improvements in CF status in 5yo and Y8 children in New Zealand and similarly-aged P1 and P7 children in Scotland.
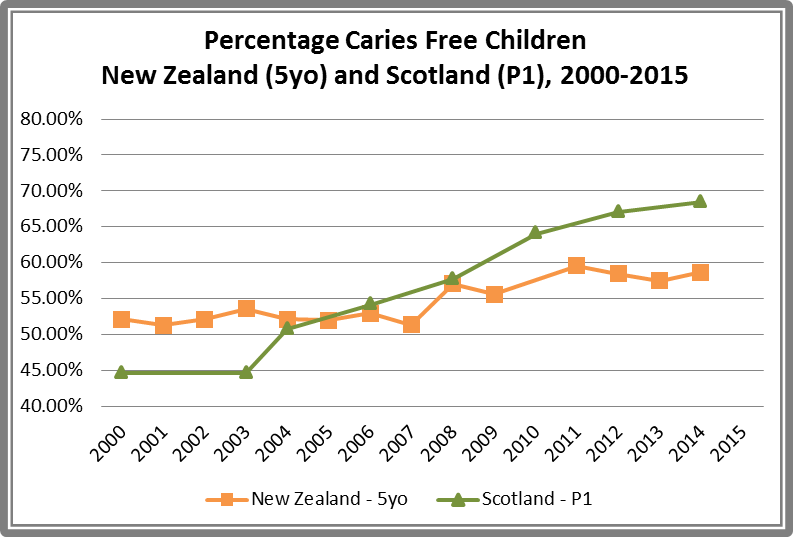
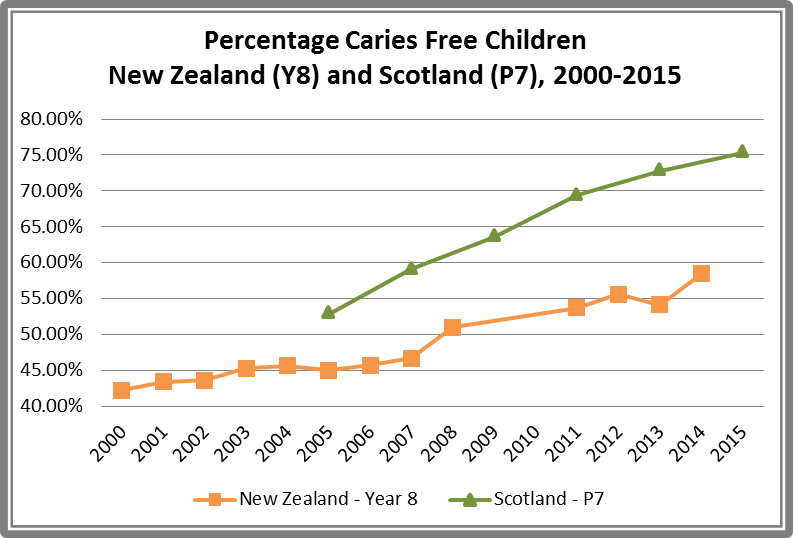
New Zealand began collecting data on children’s oral health in 1990, when 51% of 5 year olds (5yo) and 36% of Year 8 (Y8) children were CF. Between 2000 and 2014 there has been a steady, modest improvement of CF status, from 52% to 59% in 5yo children and from 42% to 58% in Y8 children. Inequalities remain, with Maori and Pacific children still bearing the heaviest burden of poor oral health.1
New Zealand started fluoridating water supplies in 1954 in Hastings. Today about 50% of the nation’s water supply is fluoridated. The Ministry of Health proposes extending mandatory water fluoridation throughout the country, believing it is the safest, most effective, and least costly way to further reduce the incidence of tooth decay.2 This decision may be based on the belief that water fluoridation is the primary – if not the only – reason for improvement in the caries-free status of New Zealand’s children.
However, a 2016 Canterbury paper raises questions about the supposed effectiveness of water fluoridation. The study found the oral health status of New Zealand’s children improved over the last decade. They also found that the differences in CF status between non-Maori children in fluoridated and non-fluoridated areas diminished. However, Maori children continue to “carry a disproportionate oral health burden, even for those in CWF regions.” The authors concluded that “CWF itself did not remove disparities in caries levels between Māori and non-Māori children. Multiple, multi-pronged strategies are needed that overcome the array of factors which disadvantage Māori.”3
The results of this study suggest that inequalities in oral health status will not decrease by simply extending water fluoridation and that a multi-pronged strategy, such as Scotland’s Childsmile program, is more likely to be effective.
SCOTLAND
Scotland began collecting children’s oral health data in 1987, when 42% of 5yo (P1) children were CF. By 2000, just before a national tooth brushing scheme was introduced, 45% were CF. Since the broader Childsmile program was introduced in 2006, levels of tooth decay have significantly and steadily fallen. In 2014 the CF-status of P1 children stood at 68%. In 2015, as show in the chart below, 75% of 11-12yo (P7) children were CF.

Most importantly, dental decay in the most severely deprived children fell from 79% in 2000 and to 55% in 2010 and continues to decline, although inequalities still exist.4
Built on the earlier tooth brushing program, Childsmile was expanded to provide a much broader four-pronged general and targeted program for all children and was fully implemented by 2010 across all Health Boards. It includes supervised tooth brushing in nursery school, targeted applications of topical fluoride in toothpaste and tooth varnishes, nutrition and oral health education, and active involvement of parents, teachers, dentists, and health providers. In addition to creating significant improvements in children’s oral health, Childsmile has also reduced inequalities across socio-economic populations and improved access to dental services, all without resorting to water fluoridation.5
COST OF ORAL HEALTH CARE IN CHILDREN BETWEEN BIRTH AND AGE 12
Scotland’s Childsmile program has produced significant improvements in children’s oral health but it is difficult to compare the cost of that program to the cost of oral health care for children in New Zealand.
NEW ZEALAND
Data for the cost of providing oral health in these age groups is not readily identifiable and has been requested from the Ministry of Health through an Official Information Request.
SCOTLAND
In 2015 Scotland’s public health minister Maureen Watt declared Childsmile was saving almost £5m a year in treatment costs and had reduced the incidence of obvious tooth decay by 14% since 2007. She said “This is a really tremendous example of spending to save. The Childsmile programme shows what can be achieved when we have a real focus on prevention – in particular in the world of public health.”6,7
That same year the University of Glasgow published an analysis of costs and projected savings associated with the Childsmile program. As shown in the chart below, since 2004 the initial nursery tooth brushing program and the 2006 Childsmile program have saved the government more than the yearly cost of implementation.
In 2010, the 8th year of the program, it is estimated that the £1,873,335 yearly cost of Childsmile saved the government £5,793,983 in averted treatment costs. The targeted approach of this preventive program is expected to continue to save money and “further improve the oral health of children in the most deprived communities, who continue to carry an additional burden of dental disease.”8
COST OF WATER FLUORIDATION
Cost effectiveness is frequently used as an argument for fluoridating drinking water, but a 2015 U.S. study refutes that argument. The U.S. Government contends that $1 spent on fluoridating water saves $38 in dental treatment costs. However, the study shows the cost benefits of fluoridation are often over-estimated due to flawed methodologies and that “The real-world costs to water treatment plants and communities are not reflected.” When such costs are included, the expected savings are substantially reduced and actually eliminated by the “estimated cost of treating dental fluorosis,” a cost borne directly by families rather than the government.9
Similarly, a 2016 Massey University paper concluding that water fluoridation remains a cost effective solution for tooth decay in New Zealand10 has been criticized by Fluoride Free NZ.11 The paper uses New Zealand’s 2009 Oral Health Survey to calculate the difference in tooth decay rates between fluoridated and non-fluoridated areas although the Survey was expressly not designed to assess dental health in relation to water fluoridation exposure.
ROLE OF EXCESSIVE FREE SUGARS INTAKE IN TOOTH DECAY
In 2015 the World Health Organization published “Sugars intake for adults and children” which advocates for significant reductions in free sugars intake to reduce tooth decay. Regarding the use of fluoride to prevent caries, it states that “Although exposure to fluoride reduces dental caries at a given age, and delays the onset of the cavitation process, it does not completely prevent dental caries, and dental caries still progresses in populations exposed to fluoride.”
Furthermore, regarding 3 population studies in Japanese children with low fluoride exposure, it was found that “lower levels of dental caries development were observed when per capita free sugars intake was less than 10 kg/person/year.” The report then states that “dental caries persists in fluoridated populations, especially in adults; therefore, all populations, irrespective of fluoride exposure, could potentially benefit from a low level of free sugars intake to protect against dental caries.”
It concludes that “The negative health effects of dental caries are cumulative because the disease is the result of lifelong exposure to the dietary risk factor (i.e. free sugars). Being free of cavities in childhood does not mean being caries-free for life, and most dental caries is now occurring in adults. Therefore, even a small reduction in risk of dental caries in childhood is of significance in later life.”12
Eating too many free sugars, found in sugary drinks and processed foods, contributes not only to tooth decay but also to malnutrition and obesity. It reduces the amount of nutrient-dense food a person eats, including the protein, fat and fat-soluble vitamins (A, D, and K2), and minerals (calcium, phosphorus, and magnesium) required for the formation and maintenance of healthy teeth. Fluoridating water does nothing to improve the underlying cause of tooth decay, malnutrition, and, as more and more research shows, is not safe or effective or cost-efficient.
CONCLUSION
Rates of tooth decay in children have fallen in many countries that don’t fluoridating their water. Eating too much sugar, and the resultant malnutrition, are major factors in causing tooth decay in both fluoridated and non-fluoridated areas. Inequalities in oral health between Maori and non-Maori children remain in spite of fluoridation, while the differences in oral health in the non-Maori population between fluoridated and non-fluoridated areas are diminishing.
Scotland’s Childsmile program is saving money while reducing tooth decay in children without resorting to water fluoridation. Before New Zealand moves forward with its goal of mandatory nation-wide community water fluoridation, it should work to reduce children’s intake of free sugars in fizzy drinks and processed foods, educate parents about the importance of healthy eating for themselves and their children, and carefully examine Scotland’s preventive Childsmile program to see how the principles of its success can be applied in New Zealand.
Proper nutrition, which means eating a nutrient-dense diet and greatly reducing the intake of free sugars, is the key to normal development of the human body. In cases where malnutrition prevents children from receiving nutrients crucial for normal tooth development, fluoride applied topically through toothpaste and fluoride varnishes can be used as a target last resort to provide some defence against tooth decay. However, unless the malnutrition itself is corrected, tooth decay will progress regardless of exposure to fluoridation. Educating prospective parents about proper nutrition and providing supervised tooth brushing in nursery school works in Scotland. It would work in New Zealand, too.
REFERENCES
- Ministry of Health, Age 5 and Year 8 oral health data from the Community Oral Health Service
- Ministry of Health, Fluoridation
- Schluter, P. J., & Lee, M. (2016). Water fluoridation and ethnic inequities in dental caries profiles of New Zealand children aged 5 and 12–13 years: analysis of national cross-sectional registry databases for the decade 2004–2013. BMC Oral Health, 16(1), 21.
- Scotland’s National Dental Inspection Programme reports
- http://www.child-smile.org.uk/
- Childsmile dental scheme ‘saves NHS £5m a year’, BBC.com, 9 June 2015
- Childsmile hailed a success
- Anopa, Yulia et al. “Improving Child Oral Health: Cost Analysis of a National Nursery Toothbrushing Programme.” Peter M. Milgrom. PLoS ONE10.8 (2015): e0136211. PMC. Web. 26 June 2016.
- Ko, Lee, and Kathleen M Thiessen. “A Critique of Recent Economic Evaluations of Community Water Fluoridation.” International Journal of Occupational and Environmental Health2 (2015): 91–120. PMC. Web. 26 June 2016.
- Fyfe, Caroline et al. “A cost effectiveness analysis of community water fluoridation in New Zealand.” NZMJ 18 December 2015, Vol 128 No 1427.
- Fluoride Free NZ. “Fluoridation is not cost effective.”
- World Health Organization, (2015) “Sugars intake for adults and children.”