Fluoridation promoters now say the primary benefit from fluoride is topical not systemic i.e. it works on the outside of the teeth not from swallowing.
The original theory that fluoride needed to be ingested so that it would be incorporated into the growing tooth enamel and hence make the teeth more resistant to decay has been thoroughly debunked and not even fluoridation promoters espouse this theory anymore.
Fluoride does get into the tooth enamel, but that does not make the teeth more resistant to decay. In fact, it causes dental fluorosis which is the first outward sign that a child has been over-exposed to fluoride (aka poisoned by fluoride). See Topical vs Systemic for more information.
Dr Robin Whyman (former Chief Oral Health Advisor and former consortium partner of the now defunct National Fluoridation Information Service) says that fluoride works by contact with the tooth surface. He then goes on to explain that when we swallow fluoride it gets into our blood stream and comes back out via our saliva providing an increased level of fluoride which is picked up in the biofilm conferring a topical benefit.
The problem with that is that fluoride saliva levels are only increased from 0.006ppm to 0.016ppm and this is not enough to confer a topical benefit.
The CDC acknowledges that fluoridated water has no cariostatic effect: “The concentration of fluoride in ductal saliva, as it is secreted from salivary glands, is low — approximately 0.016 parts per million (ppm) in areas where drinking water is fluoridated and 0.006 ppm in nonfluoridated areas . This concentration of fluoride is not likely to affect cariogenic activity.” (CDC MMWR)
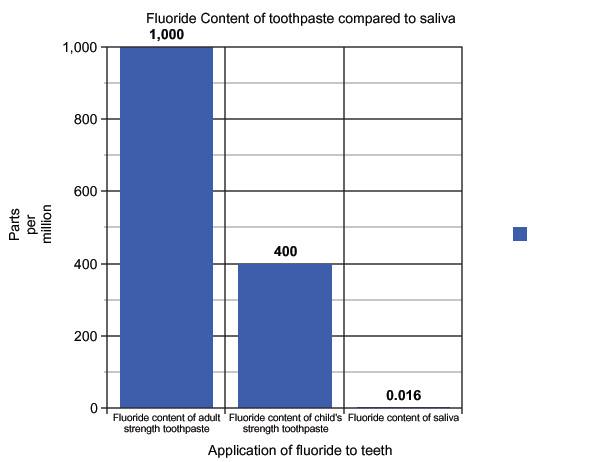
So we have now stepped into the twilight zone? We have fluoridation promoters, such as Dr Whyman, advocating that everyone use adult strength fluoride toothpaste at 1000pm because child strength at 400pm is not strong enough to provide a topical benefit, whilst at the same time telling people they should drink fluoridated water so that 0.016ppm can be secreted from the salivary glands to provide a topical benefit.
Apart from the fact that this is patently absurd, there is no scientific evidence to support that low amounts throughout the day will confer any benefit. This claim appears to simply be the only way of hanging onto fluoridation policy.
The following studies show that fluoridated water is too low in fluoride to provide any topical benefit:
1. Damato, F.A. (1990). “Effect of fluoride concentration on remineralization of carious enamel.” Caries Res. 24(3):174-80
2. Cutress, T.W. (1995) “Effects of fluoride-supplemented sucrose on experimental dental caries.” Advances in Dental Research 9(1).(Note – Cuttress is a NZer)
3. Arends, J, Christoffersen, J, Ruben, J & Jongebloed, WL (1989) “Remineralisation of bovine dentine in vitro. The influence of the F content in solution on mineral distribution.” Caries Res. 23. 309-14.
4. Pearce, E.I. (1992). Supplementation of domestic sugar (sucrose) with fluoride. New Zealand Dent. J. 88(393):84-8.
5. Tanaka, M. (1993). “Effect of fluoride incorporation into human dental enamel on its demineralization in vitro.” Arch Oral Biol. 38(10):863-9.
References provided by Dr Whyman
Dr Whyman provided the following references as supporting topical benefit from fluoridated water:
1. Featherstone J D, Glena R, Shariati M, Shields C P “Dependence of in vitro demineralization of Apatite and Remineralization of dental Enamel on Fluoride Concentration” J Dent Res 1990 Feb; 69 Spec No: 620-5; discussion 634-6
2. ten Cate J M, Featherstone J D “Mechanistic Aspects of the Interactions Between Fluoride and Dental Enamel” Cit rev Oral Biol Med 1991;2(3):283-96
3. Featherstone J D “The Science and Practice of Caries Prevention” JADA 2000, Vol 131, No 7, 887-899
4. Ole Fejerskov, Anders Thylstrup, Mogens Joost Larsen “Rational Use of Fluorides in Caries Prevention” Acta Odontologica Scandinavica, 1981 Vol 39, No. 4: 241-249.
5. Oliveby A, Twetman S, Ekstrand J “Diurnal Fluoride Concentration in Whole saliva in Children living in a high- and low-fluoride Area” caries Res 1990; 24(1): 44-7
6. Wilson A C, Bawden J W “Salivary Fluoride Concentrations in Children with various Systemic Fluoride Exposures” Pediatric Dentistry 1991; 13:103-105
7. Cutress T W, Coote G E, Shu M, Pearce E I “Fluoride Content of the Enamel and Dentine of Human Premolars prior to and Following the Introduction of Fluoridation into New Zealand” Caries Res 1991; 30(3). 204-212
8. Garcia-Godoy and Hicks M J “Maintaining the integrity of the enamel surface. The role of dental biofilm. Saliva, and preventive agents in enamel demineralization and remineralization” JADA, 2008, Vol 139, No. suppl_2, 255 – 345
Critique of the references
We have obtained copies of only two of these studies.
Number 7 (Cutress et al). Not only does this study NOT ADDRESS the means by which fluoride gets into tooth enamel, it quite clearly states its assumption that it is by systemic incorporation. In no way does it support Dr. Whyman’s claim. Either Dr. Whyman has never read this study, or he is deliberately bluffing.
Number 2 (Ten Cate and Featherstone). This study found topical benefit to dead tooth enamel in vitro, but acknowledged that tooth enamel in the mouth behaves differently, and therefore the results could not be claimed applicable to live teeth subjected to fluoridated water.
Number 1 and 2 Regarding the studies, we note that studies one and two were by Featherstone, before his 1999 publication, which refutes topical benefit from fluoridated water.
Number 3 We understand number 3 is a variation of his 1999 publication, so it is highly unlikely that he states a reversed his position in that timeframe.
Numbers 4 to 6 predate Featherstone’s 1999 publication, which refutes them.
Number 8 We are unable to comment.
However, given there are 5 studies clearly showing that fluoridated water has no topical benefit, and that the two references we have been able to check do not support topical benefit from fluoridation, the balance of science today must be taken that it does not, unless NFIS can provide the other studies for the Society’s examination. To date they have refused to supply them, on the grounds of copyright. (2013)